|
‘But are we to compete? And is not that idea of competition the very mistake we are all making?’ Sir Ernest Morris, 1934 (House Governor, The London Hospital) In medical terms the inter-war period was essentially one of consolidation. Methods of clinical investigation and surgical techniques improved, radium and radiotherapy became accepted in the management of cancer, and there were several major advances in therapeutics like the introduction of insulin in 1922, sulphonamides in 1935 and blood transfusion services in 1937. Medical education improved as clinical units of a university nature were introduced into a number of London medical schools, and much thought was devoted to postgraduate education. Hospital organisation and finance became critical issues. The financial crisis of 1920 slowed the campaign to break up the poor law, and was responsible for a drive for ‘value for money’ by coordinating the voluntary and poor law hospital systems which sometimes competed and always overlapped with each other. Ideas which had previously appeared almost revolutionary achieved a degree of respectability, and to overcome rivalries the organisation of all hospitals into a single system was suggested. Money being short, cooperation became the watchword. The creation of the Ministry of Health in 1919, at the end of a hard fought inter-departmental struggle, was in some ways symbolic of new approaches to the provision of health care.1 The Fabians had pointed to the confusion which existed between the health care activities of different government departments, the Local Government Board, the Board of Education, the Privy Council and the Home Office. The new Ministry gathered these functions together, under a Minister who was himself a doctor and a secretary and chief medical officer with deep understanding of medical and political realities. Sir George Newman, the chief medical officer, said that the Ministry reflected an understanding of the need to apply the principles of preventive medicine to the whole population. No longer would individual families receive services from several different organisations, which each worked in water-tight compartments ‘along lines which never met, covering the ground, or part of the ground, that others covered’.2 The Ministry of Health had set an example in collaboration, and there was a political will to achieve cooperation between the hospitals as well. The new Ministry was given a guarded welcome by The Lancet and the British Medical Association, but its formation was seen in some quarters as a first move towards a state hospital service.3,4The Minister, Dr Christopher Addison, reassured the hospitals that there was no intention of enforcing any particular principle or doctrine. But some senior civil servants, impressed by the organisational opportunities open to local government, saw the possibility of a chain of hospitals, united by motor transport, under local authority control. Taken to the limit, cooperation could eventually lead to the unified county medical service described by the Webbs, encompassing the health functions of local authorities, those provided under the poor law, and the voluntary hospitals great and small. The British Hospitals Association, a successor to the old Hospitals Association, organised a conference at St Thomas’s to consider the relationship of the voluntary hospitals to the new Ministry of Health. The association’s secretary, Mr Buchanan, circulated a paper stating that the hospitals with their special and general departments, and their medical and nursing schools, must be maintained at the highest possible standard. A connecting link with the public hospitals was however necessary. The Association and The Lancet both agreed that the voluntary hospitals must be allowed to continue their great work, which stemmed from the individual freedom of the hospitals to undertake any enterprise which seemed to promise well.5 The experiences of the Great War demonstrated the form the connecting link might take. Men like Sir Robert Jones had developed systems allowing war wounded and soldiers with fractures to be evacuated for treatment, and doctors returning from the Forces had demonstrated their ability to plan and administer large medical organisations, cooperating in the provision of a unified service. Amongst them was Major General Sir Bertrand Dawson, physician to The London Hospital. In his Cavendish Lectures to the West London Medico-Chirugical Society and during debates about the future of the medical profession held at the Royal Society of Medicine in 1918, Dawson maintained that an efficient service could not be self-supporting. Men and equipment must be distributed according to the needs of the community. Local hospitals and clinics should be related to central hospitals in larger towns which would provide specialist services. These in turn might be subordinate to a larger provincial hospital, and all would be maintained by a health authority. Only the teaching hospitals might stand apart, for ‘they served the nation whilst other hospitals served a town or county’.1,6 Dawson pointed to the growing realisation that much disease was preventable and that the best means of preserving health and curing disease should be available to all as a right rather than by favour. He thought that administrative matters should be determined by a board consisting of lay and medical members; professional and technical questions by doctors alone. War service had taught the medical profession many lessons. During the early years of the war Dawson discussed grouping and regionalisation of hospitals, and later when he chaired the Council on Medical and Allied Services the military organisation of the country into ‘commands’ was seen as a possible model for health service organisation.6 (see map below)
At the end of the war the financial position of the voluntary system was weak. Hospital subscriptions from the middle classes had declined and the formation of the Ministry of Health had led some to assume that the needs of the hospitals would soon be met in other ways. The voluntary hospitals no longer received payment for the treatment of war-wounded. Initially the hospitals had been worried about the acceptance of government support, for it breached the voluntary principle to receive state aid. The withdrawal of these funds left the hospitals in difficulty. Inflation during the war had increased hospital costs considerably. The King’s Fund’s distribution committee was particularly concerned with the expenditure of The London Hospital, which was the subject of a special report. Its costs had risen faster than those of the other great London hospitals. In vain did Lord Knutsford protest that his hospital treated more patients per bed than any other, and that the length of stay was the shortest. Many hospitals had deficits despite the contributions made by local authorities as part of schemes for treating tuberculosis and venereal disease. In recognition of the problems the grants made by the King’s Fund in 1918 were increased, and were the largest in the Fund’s history. In spite of the difficulties a number of hospitals were preparing schemes for extension, which seemed to many a good form of war memorial. The annual report of the Fund for 1918 pointed out that the combined effect of many developments, good though they might be individually, would be to add a large number of beds to the total in London. The Fund feared that the revenue available would not increase in parallel, and that the problem of closed beds which it had dealt with successfully at the turn of the century would emerge once more. The new beds might not be provided in the areas needing them most; the Fund therefore asked all hospitals to state what was proposed, for it believed that one of the advantages of a central fund was that it could form a clearing house for ideas of this type. Detailed enquiries were made about the ability of hospitals to support proposed extensions, in an attempt to ensure that beds once provided could be used, and that the new extensions reduced the worst inequalities of provision. By 1920 extensions totalling 3,445 beds were contemplated. Of these only 1,489 were ‘passed’ by the distribution committee, and were therefore eligible for support by the King’s Fund. (see table 15 below). With perception based upon long experience, Henry Burdett had written in 1893 of the danger a voluntary hospital faced as its work expanded.
‘Many instances might be quoted in the history of the world where a hospital originally supported on the voluntary system with adequate funds provided from the revenues derived from the original endowment, has gradually become hopelessly involved owing to the increase in population resulting in increased demands on its resources. Where this has occurred the government has often-stepped in, first of all with temporary assistance or a special grant, to be followed later by further and larger contributions from State funds with representation in management, and ultimately by the practical taking over of the institution, and the absorption of its revenues by the State.' 7 Burdett repeated this warning in the thirtieth edition of Hospitals and Charities, the last he edited before his death in 1920. He sensed ‘a sinister attempt for what would appear to be political motives to maintain that the voluntary system had failed,’ and to substitute a state system.8 The Labour Party did in fact believe that, solvent or not, the voluntary system could never meet all needs adequately. It believed that local authorities should establish their own hospitals and, as a dual system would create problems, the voluntary hospitals should be absorbed. Hospitals in London and the university towns with a national and even international reputation should be funded and administered directly by the Ministry of Health, but there should also be a system of large central local authority hospitals linked to smaller local and cottage hospitals.9’16 Matters came to a climax in 1920. Notwithstanding an emergency distribution of £250,000 by the King’s Fund and a further £250,000 from surplus funds of the Red Cross and St John’s, it seemed improbable that the voluntary hospitals could continue on their traditional basis unless immediate steps were taken to re-establish the pre-war position. The King’s Fund decided to draw upon its capital resources, but Hospital Sunday did not do so. On 26 January 1921 the King’s Fund considered and ratified its policy for the preservation of the voluntary hospital system.10 The propositions the Fund advanced were that the voluntary system was the most effective and cheapest method of providing the best treatment and advancing medical knowledge and practice; that at least a substantial part of the cost should be met by voluntary contributions; that the current receipts were inadequate to meet the present cost, let alone the debts of the London hospitals, or the need for redevelopment; but that no remedy should be contemplated which reduced voluntary contributions or removed independence of management. It was proposed that payment by patients, insurance schemes, and grants-in-aid by public authorities for specific work should be considered. Block grants were however deprecated, although pro-rata assistance was a possibility. The Lancet agreed that it was the duty of the state to supplement rather than supplant the voluntary hospitals, and to provide the care needed by many who were not ‘an object of charity in the normal sense’. State support should not, however, deprive the hospitals of their independence of control.11
The years 1921-24 were a period of
continuing difficulty for the hospitals, and the possibility of the
breakdown of the great voluntary hospitals and their medical schools
led the government to establish the Cave committee, which first met
in January 1921. The committee agreed that there was great merit in
the voluntary system, that it was
in the public interest to maintain it, Continuing pressure to reduce public expenditure led ti the ‘Geddes axe’. The government decided to provide no more than £500,000, and to give state assistance for a limited period only, simply to allow the voluntary hospitals a breathing space so that they could re-establish their position.13 The voluntary movement would have to meet some of the deficit itself, perhaps on a pound-for-pound basis. The Hospitals Commission recommended by the Cave committee was formed, under the chairmanship of Lord Onslow, and it supervised the distribution of the government’s £500,000 grant. A leader in The Times criticised the Minister for his parsimony and accused his department of seeking a ‘great new experiment in State or municipal hospitalization’. Letters were published from The London Hospital and St Mary’s, drawing attention to the plight of the hospitals.14 His Majesty himself asked the Ministry for reassurance about the position of the London hospitals. In reply the Minister said that the first principle in the government’s mind was that the voluntary system must be maintained in full force and vigour. Had he been so foolish as to wish to destroy the voluntary hospitals no surer way could have been found than unconditional deficiency grants. Voluntary support would then have diminished, state contributions would have risen by leaps and bounds and state control would have followed. The Minister’s letters were difficult to draft. As he pointed out in a personal letter to the editor of The Times, painting the blackest possible picture was a traditional way of stimulating voluntary support. The Minister could say nothing which would reduce the ability of the hospitals to raise money.13 A combined hospitals’ appeal by the King’s Fund which aimed to stabilize the hospitals’ financial position raised £480,000 fairly rapidly.15 The Labour Party used the opportunity of the financial crisis to re-state its hospital policy16 and advanced thirteen propositions which it believed should form the basis of a future hospital service. By 1924 the financial problems were easing and the King’s Fund could report that the deficits of the London hospitals were becoming smaller each year. Hospital savings schemes had been inaugurated, and many hospitals could once more balance their books. In April 1924 a conference was held under the auspices of the Labour Party, attended by a wide variety of organisations including the British Medical Association, the voluntary hospitals and members of professional staff associations. The conference was called to discuss the desirability of further state aid to extend and maintain the hospitals. In sending the conference his good wishes, the Prime Minister, Mr Ramsay MacDonald, said that the problems of the hospital system, if the existing chaos could be so described, was a symptom of inadequate civic organisation. It fell far short of the achievement its friends and supporters desired. He hoped that a common and wise policy might be the outcome of the discussions. Speakers from the left maintained that great though the efforts of the voluntary movement had been, it had failed to provide completely what the nation needed. The only way out of the impasse was for the state to accept the responsibility of providing hospital treatment for all who needed it, transferring the poor law infirmaries to the local authorities, and giving the voluntary hospitals the choice of remaining as they were, or of coming to an arrangement with the local health authority. Lord Knutsford, however, thought that the record of the state in providing health care for the poor and the armed services showed that whilst it might do its bare duty, it would be done without grace. Turning to the Labour Party policy, he spoke scathingly about the statements which had been made. Hospitals were not pauperising agencies, patients were not admitted preferentially if they could pay something towards the cost of their treatment, neither were they afraid of entering hospital because they might be subject to experimental treatment. The voluntary hospitals abided by the Sermon on the Mount, not the cold code of the Charity Organisation Society. Lord Knutsford tartly remarked that the Charity Organisation Society had nothing to do with charity. The best plan would be to strengthen what was admittedly good, and not change to a system of state management which would satisfy nobody.17 Lord Somerleyton, representing the King’s Fund, pointed to the improving financial position of the hospitals as a result of their steady efforts, and the final resolutions, passed by the conference without dissent, called for increased support and public assistance for the voluntary hospitals to preserve the best features of the voluntary system, a closer relationship between public and voluntary hospitals, improved geographic distribution, cooperation between the various institutions, and the ‘removal of all taint of the Poor Law from the infirmaries, throwing them open to all citizens’.17 Similar sentiments were expressed at a conference of the British Hospitals Association, and a conference of Local Voluntary Hospital Committees which had been established to work with the Onslow Commission. It was announced in the House in February 1924 that the Onslow Commission was to seek evidence of the need for additional hospital accommodation, and the best means of providing and maintaining it. Most hospitals, although their financial problems were lessening, were still without the means to extend their facilities. The King’s Fund pointed out the difficulty of trying to determine need for beds from information such as waiting list size, and the replies it received from the London hospitals only permitted an estimate of the number of beds which came into the range of ‘practicable possibilities’. These were beds which would fit into the general pattern of provision, and which could conceivably be funded either at once or in the foreseeable future. The increase amounted to about 2,000 - to something a little over 15,000 in all.18 The Onslow Commission reported that even when the use of available Poor Law beds had been taken into consideration a shortage of beds existed. It favoured state grants towards building costs and a further measure of assistance to help the hospitals to overcome their arrears. However the government would provide no further money and the commission was disbanded in 1928. The financial recommendations of the Cave committee and the inauguration of hospital savings schemes brought about considerable changes in the financing of voluntary hospitals. The needy continued to receive free treatment — the primary function of the hospitals — but it became usual to charge the more affluent. Financial organisation was increasingly based upon payment for services rendered.20’21 The King’s Fund had emerged from the financial crisis more powerful than ever as the spokesman for London’s hospitals. In its evidence to the Onslow Commission it had said that it could fulfil the role of a central administrative body and cooperate with other coordinating bodies on the outskirts of London. It had channelled not only voluntary subscriptions but state grants to the hospitals; and being voluntary itself it respected the independence of the hospitals. Charing Cross Hospital, in its own evidence, suggested that the Fund be given still greater power ‘to smash the hospitals into line as regards expenditure or amalgamation’. Such a dictatorial approach was not the Fund’s way of working. At the zenith of its power, its ‘friendly persuasion’ was seldom ignored. The voluntaries were keenly aware of the need to retain public sympathy if their financial and political interests were to be safeguarded. The King’s Fund established a propaganda committee in 1924 to arrange lectures and produce leaflets and films. Exhibition displays were constructed and a miniature hospital was built to 1/16th scale, complete with a royal statue.22One parent claimed that his son’s eye had been injured by an ultra-violet lamp in a display of modern hospital equipment. A film was made called ‘A Hundred Years of Progress’, and Ernest Morris, house governor of The London, delivered lectures on the pros and cons of nationalisation of the hospital service. Developments in medical education The recommendations of the Haldane Commission has been overtaken by the Great War. InJune 1918 Sir George Newman, chief medical officer of the Board of Education and later the first chief medical officer of the Ministry of Health, submitted a report on medical education to his Board.23 He expressed some diffidence in writing upon the subject, but in a carefully constructed document he proceeded to review the nature of university education and to identify four main deficiencies. They were teaching at a level below university standard; failure of university departments to work with each other; inadequate medical research within the teaching system; and the need for better postgraduate education. The following year grants became available from the Board of Education to assist the establishment of clinical professorial departments where academic staff would work full-time in teaching and research, undertaking no private practice. St Bartholomew’s Hospital had already decided to establish such a unit without waiting for further developments. A unit was also established at St Thomas’s, and University College Hospital received a magnificent gift of £1,205,000 from the Rockefeller Trust for the same purpose. Academic units would not be concentrated into a few university-dominated hospitals as Haldane had envisaged, but would be widely distributed. Some schools, like Guy’s, chose to maintain the traditional pattern and after the first units were established progress was slow. In its evidence to the Goodenough committee in 1942 the University of London listed those professorial units in existence at the outbreak of war in 1939; none existed in half of the London medical schools.
The academic staff were very much in the minority amongst the honorary consultants, and each professorial unit needed at least fifty beds, inevitably at the expense of the other clinicians who continued to teach students, but who no longer had the field to themselves. Slowly the schools began to move closer towards university-based education, and to adopt the pattern of organisation outlined by Sir William Osler in 191124 The University of London came to the conclusion that the minimum number of beds essential to have an efficient medical school was 600, and every medical school came under pressure to increase its laboratories and service departments. Hospitals and schools could not function as they had once done with little more than a number of wards and an operating theatre. Another problem involved medical education for women. The establishment of the London School of Medicine for Women in 1874, in association with the Royal Free Hospital, was followed during the Great War by the admission of women to the majority of medical schools in London. After the war most hospitals reverted to their pre-war tradition, and clinical places were once more difficult to find in London. Poor law reform and the boards of guardians Amongst many other objectives the long campaign to reform the Poor Law aimed to achieve the transfer of infirmaries from boards of guardians to local authorities. Ever since the 1830s there had been increasing dissatisfaction with infirmary management, which varied from the enlightened to the apathetic. Mr Joseph Chamberlain, speaking in 1888 during the second reading of the Local Government Bill, suggested the inclusion of Poor Law administration amongst the duties of the new county councils.25 However boards of guardians remained untouched, as they did ten years later when the London Government Act (1899) abolished the vestries and created twenty eight London boroughs. The Royal Commission on the Poor Laws (1909) had pointed to the overlapping of hospital authorities, and the Majority and Minority Reports had agreed that boards of guardians should be abolished. The Maclean committee, established at the end of the Great War to consider the post-war planning of health services, also supported the transfer of functions.2 The Maclean committee pulled together the points on which the Majority and the Minority Reports had been agreed, and Sir Robert Morant, a senior civil servant with extensive experience of both health and education, added a note to say that he assumed that all the main forms of medical service would be brought together under one Minister, within a Ministry of Health, before such a transfer took place. This happened, the Ministry of Health being formed in 1919, but whilst the transfer of functions became accepted policy, the change was not to the liking of those to be abolished — the boards of guardians and the Metropolitan Asylums Board. Although Burdett had little respect for state or municipal management, he wrote in the introduction to the 1919 edition of Hospitals and Charities that he looked forward to the time when county councils would take over the administration of the entire poor law system. Such a reform would make it possible to classify sick and healthy paupers, and persuade public opinion to insist on the best possible provision being made for pauper patients.8 Burdett also believed that the transfer would make it possible to provide better staff and equipment, to construct outpatient departments, and provide patients in London with the additional accommodation which was needed, particularly away from the centre ‘in the areas where the working classes live’. London infirmary medical superintendents also supported transfer to the London County Council on the grounds of economy, better distribution of patients between institutions, the likelihood that better candidates would be attracted to the medical and nursing services, and the opportunity which would be created to develop specialised services. The superintendents envisaged district hospitals, providing one bed per 300 population, with associated outpatient departments. There would also be special institutions for ophthalmology, ear, nose and throat disease, tuberculosis, orthopaedics, fevers and radiotherapy.26 The Maclean report had suggested that among the functions to be transferred to the London County Council should be those of the Metropolitan Asylums Board. The London County Council agreed, believing that the health functions which were carried out by many different bodies should be united under its control, just as Parliament had united governmental health activities in a single Ministry. The Clerk was asked to report on the health functions of local authorities and other bodies in London, and the report recommended that the council should be the sole and central institutional body for health services in London.27 It was adopted by the London County Council in December 1919, for it was consistent with the general thrust of council policy to extend its sphere of influence and centralise control. The council made cordial reference to the work of the Metropolitan Asylums Board and suggested that its institutions and its highly competent staff should be transferred en bloc. The council also suggested that the voluntary hospitals should establish a central voluntary hospital council with which it might negotiate, and sought a meeting with the new Minister of Health. The representatives of the council were received by the Minister on 23 April 1920. Dr Christopher Addison had previous experience of the council’s ambitions, in the housing field. Nevertheless after the council had presented its case he said it was clear that a good deal of muddle had arisen from the needless multiplication of authorities. While some services were best administered locally, others were not. The more specialised the services, the wider the range of the responsible authority had to be, and it was essential to have an authority to deal with some services over a considerable area. The Minister felt that the council’s main principles were unassailable.28 For the next twenty-five years the Ministry and its officers came to turn, more or less automatically, to local government when an extension of social services was envisaged. Because of the financial crises of the early twenties, and public campaigns for a reduction in government expenditure, there was considerable delay before proposals for Poor Law reform could be considered. They were not circulated to boards of guardians and the Metropolitan Asylums Board until January 1926. It was proposed to abolish boards of guardians and with them the Metropolitan Asylums Board which derived its membership from ‘destitution authorities’. In London the County Council would become the supervising and controlling authority for all health purposes throughout the administrative county, which covered essentially the same area as the Asylums Board. In its reply the Metropolitan Asylums Board stated that it was convinced that the London County Council would find it impracticable to undertake the enormous task of managing all the hospitals and institutions involved, and that an independent body was justified.29, 30 Neville Chamberlain and collaboration
In 1919 Sir Bertrand Dawson was commissioned by the new Ministry of
Health to chair a council to advise on the systematised provision of
health services. (the Dawson report is considered in more detail in
the subsequent section) The
report proposed, with a good deal of post-war
fervour, the linkage of hospitals into a single system. At the time
it did not carry much weight. It was common knowledge that there was
a substantial body of disagreement amongst the interests represented
upon the council, and that the report had been prepared within a
tight time limit. The report, admittedly an interim one, ignored
costs, the existing system of local government, and the pat Neville Chamberlain did not believe that the voluntary hospitals should suffer extinction or come under state control, although he was often accused of wanting to take them over. However he told an audience in Coventry in October 1926 that public heath provision could not be looked at in water-tight compartments. The voluntary hospitals should consider how they might fit into the wider scheme of things. Could cooperation be extended? Might there not be in time some central health authority with representatives of the voluntary hospitals upon it, responsible for the general health policy of an area? In return for a certain subordination of their complete and absolute freedom to do what they liked, they might receive financial assistance.13 His speech revived fears of a state take-over and The Times published a leading article criticising his approach. Chamberlain replied that he was concerned with overlapping services and waste of money. Local areas should be examined as a whole, and closer coordination of the institutions in an area by a central body with general powers of guidance was needed. Would not the voluntary hospitals like to play their part? If they did not, such a body would undoubtedly be formed without them, a development he would view with grave anxiety.33 The British Hospitals Association wrote to Chamberlain to ask how the voluntary hospitals might best cooperate with the public health services. Chamberlain considered that discussions might be more productive if there was a series of concrete proposals to be considered, rather than the somewhat abstract topic of ‘cooperation’. He therefore suggested a number of issues which might be considered locally, including the allocation of some categories of illness to one or other type of hospital, the effect of such agreements on future hospital development, the deficiencies which existed and how they could be remedied, the possibility of a clearing house for admissions, so that patients could be admitted rapidly to one or another institution, and what pattern of joint staffing might be desirable.33 Chamberlain was invited to address the association but declined because of the uncertainties surrounding the forthcoming Local Government Bill. The British Hospitals Association consulted its branches and replied to the Minister’s questions without being particularly constructive. Cooperation on building developments did not seem to them to be practicable. The voluntary hospitals already provided a full service, and where they did not they planned to do so, but it would help if their staff could use beds in public hospitals. Dawson, now in the House of Lords, used his influence within the British Medical Association to ensure that its response was more constructive. In 1927 Neville Chamberlain addressed the autumn meeting of the British Medical Association on cooperation between the voluntary system and the municipal hospitals34, and made further attempts to persuade the British Hospitals Association to look seriously at the need for it. In response the Association’s officers told their members that it was imperative that the voluntary hospitals should cooperate with local authorities. The Local Government Bill would soon be law, and if competition developed with the rate-supported hospitals, which had almost unlimited finance behind them, there could be only one outcome. Yet the very thought of cooperation alarmed many of the voluntary hospitals. Eason, the medical superintendent of Guy’s, referred to the elephant who said he was a strong believer in cooperation as he sat on the pheasant’s eggs in a praise-worthy attempt to assist in hatching them out. Some of those who worked for the voluntary hospitals feared that they would be squeezed out of existence by a beneficent public sector. Informal contacts were established between the London voluntary hospitals and the county council’s medical officer of health, Dr F N K Menzies, (later Sir Frederick Menzies) who began to play an increasing role in hospital affairs. He was described as a big man, mentally and physically, full of vigour and initiative, with a pleasing personality. He had a commanding presence, a persuasive tongue and personal friendships in high places. The Lancet regarded him as a man of affairs with great driving power, a facility for choosing the right assistants and a knack of getting his way in large scale problems of medical administration.36,37 Already an honorary member of the Westminster Hospital’s staff, he met representatives of the voluntary hospitals and assured them that the London County Council was not seeking to take them over. At a meeting with the King’s Fund in 1928 Menzies said that the attitude of the county council was entirely friendly and a tradition of cooperation with voluntary hospitals had been established. However the hospitals should bear in mind that if satisfactory arrangements were not agreed, the Labour group would demand complete municipalisation and would be able to make out a good case. An assumption of arrogance on the part of the voluntary hospitals would only antagonise their friends and throw them into the hands of their enemies. The King’s Fund became convinced that Menzies was a valuable ally, but recognised that if the voluntary hospitals showed an unwillingness to negotiate his patience might become exhausted.10 The British Hospitals Association organised two conferences of London hospitals, for those with and those without medical schools, to discuss the future with Menzies. The teaching hospitals expressed doubt about the ability of the council to manage the vast hospital resources to be transferred to it, and if it tried it might be difficult to avoid antagonism, competition and duplication between the two systems. The voluntaries suggested that the county council could ask them to manage municipal hospitals on its behalf and at its expense. A variety of agency arrangements were possible and existing examples of cooperation were cited. St Mary’s students went to the Paddington Infirmary, and the Infirmary used St Mary’s laboratories. The chairman of the guardians was a member of the St Mary’s board, and the benefits of the association were mutual. Dr Menzies could not agree that the council might consider surrendering its responsibilities, although Herbert Eason, the medical superintendent at Guy’s, repeated the proposal that teaching hospitals could administer the municipal hospitals and deploy their staff in both, at a meeting of the British Medical Association chaired by Menzies in 1927. 35, 39 Two doctors wrote to The Times suggesting an advisory council for hospital services in the metropolitan area, in which the representatives of the voluntary hospitals would be in the majority (because of their long experience) and in which the King’s Fund would play a leading role. There was little support for the idea in any quarter. Meanwhile the King’s Fund established a special committee to consider the steps which should be taken whilst the Local Government Bill was passing through Parliament. The Minister, Neville Chamberlain, saw a deputation from the Fund in November 1928. He was asked if he would make it mandatory for local authorities to co-opt persons with voluntary hospital experience onto their public assistance committees. Chamberlain said that he was all for maintaining the voluntary system, and for coordination, but that he had not met with much response, being suspected of wishing to introduce municipalisation. The danger to the voluntary hospitals did not come from the Bill, but from the progressive improvement of the poor law infirmaries. Co-option would not of itself secure coordination, and would be resented by many local authorities. Furthermore, if it was made reciprocal, with the co-option of local authority representatives onto the boards of the voluntary hospitals, that also might meet with a hostile reception.10, 38,40. A series of informal discussions took place between representatives of the King’s Fund, the London County Council and the voluntary hospitals to explore the problems of working together. In March 1929 the King’s Fund published a carefully drafted memorandum on the Relations between Voluntary and Municipal Hospitals.41 It proposed permanent consultative machinery to consider hospital provision, equipment, staffing and training. It wished representatives of the voluntary hospitals to be appointed to local authority public assistance committees, proposed the coordination of the two hospital systems in nurse training, and the use of the facilities of the municipal hospitals for medical student education. The Local Government Act, as passed in 1929, included a clause placing a duty on local authorities to consult a committee representative of the governing bodies and medical staff of the voluntary hospitals about the accommodation to be provided and the purposes for which it was to be used. ‘It is imperative’, said a Ministry circular, ‘that the Local Authorities establish the most cordial relationships with, and should make full use of, the medical profession in regard to hospitals.’42 In March 1929, shortly the Bill became law, the London County Council wrote to the King’s Fund asking for its views on the manner of cooperation. The Fund had been discussing the matter with the voluntary hospitals and produced a proposal for a group which Dr Menzies felt was too cumbersome to allow any business to be done. Nevertheless the London Voluntary Hospitals Committee was formed along complex lines, representative of the King’s Fund, the Conference of Teaching Hospitals and the London Regional Committee of the British Hospitals Association.40 The Local Government Act (1929) A useful reference to the appropriation of poor law hospitals nationally is to be found at
Med Hist. 2006
January 1; 50(1):
3–28 The Development of Municipal General Hospitals
in English County Boroughs in the 1930s; Alysa Levene,
Martin Powell and John Stewart
The Act had three main effects on hospital services. It brought poor law infirmaries and fever hospitals into line with other municipal services, opening them to all in need without the stigma of the poor law. It placed them under elected and representative local authorities, instead of ad hoc bodies like boards of guardians. Finally, it decentralised the financing of these hospitals, consolidating the exchequer grants for the total range of local public services. Speaking to the medical students of the Westminster Hospital, Dr Menzies explained how public opinion had rebelled against the way a sick person had to be regarded as a pauper if he was to be treated by the guardians. Twenty-five years of agitation had at last been successful and the London County Council would soon have 75,000 beds under its control for all types of disease, five times as many as in the voluntary hospitals of London. The principle had been established that sick people in need of treatment should receive it, and if they were unable to provide for it themselves it was the business of the health authority to do so. Menzies recognised the fear of the voluntary hospitals that they would be adversely affected but he saw no reason for anxiety. For twenty years the policy of the London County Council had been cordial cooperation with the voluntary hospitals, and in its new task the council would need the sympathy and support of all who were interested in the care of the sick.43 Sir George Newman, in his annual report at the Ministry, also welcomed the change. ‘For the first time in the history of the public health services the medical officer of health has a direct and ample opportunity for closely and effectually coordinating in his area all the varied medical services of the State.’ ‘Only the best must be good enough for the patients in our Hospitals and in medical treatment expenditure is very often the best form of economy’, wrote Lewis Silkin in a London municipal pamphlet produced by the Labour Party. The London County Council intended that the hospitals to be taken over from the guardians should be used primarily as general hospitals, ‘equivalent to the voluntary general hospitals’. The council would not only possess the majority of beds in London but the biggest hospitals as well: Lambeth, St Giles’ Camberwell and St Mary’s Islington”, The voluntary movement observed the behaviour of the council with apprehension. The council could have continued to administer the infirmaries under the Poor Law Acts but it chose to work under the Public Health Acts instead, which had the advantage for the council that ‘appropriated hospitals’ were removed from the detailed oversight of the Ministry of Health.45 The council’s inheritance Developments in the infirmaries had been patchy although the use of some as military hospitals had led to an improvement of facilities. An increasing number were recognised by the General Nursing Council for nurse training and some had been opened to medical students from nearby teaching hospitals. The Paddington board of guardians had made an agreement with St Mary’s in 1920, and King’s College Hospital and the Camberwell Infirmary were in negotiation. Some infirmaries had developed considerable esprit de corps and opposed transfer to the London County Council as a threat to their individuality. The Lambeth guardians had purchased both radium and deep X-ray equipment, and had sent their senior physician on a tour of Europe to see what was being done in the world of radiotherapy.46 However, few staff of the voluntary hospitals set foot in the infirmaries; some of those who did had had their views confirmed that they provided a second class service with second class staff. The infirmaries were managed by 25 unions. Populations varied from 100,000 to 300,000, with exception of one very large union - Wandsworth. In total, they provided 16,250 beds staffed by 140 doctors. In 1928, Drs Meredith Richards and Manby surveyed the infirmaries for the Ministry of Health.47 Some of the accommodation was found to be excellent, much was indifferent, but most was found to be sufficiently good to serve a purpose. Many infirmaries were on noisy sites, had insufficient isolation accommodation, and did not classify patients according to their needs. Occasionally wards were tightly packed and there might be no margin of beds for emergencies. The surveyors thought that if existing poor law boundaries were disregarded, the facilities could be used to greater advantage. Admission policies also varied. ‘If they did not go out into the Highways and Hedges to compel patients to come in,’ said the surveyors, some guardians ‘were at least ready to welcome all who sought admission.’ Others, acting strictly within their statutory authority, made careful enquiries about the needs and resources of those seeking relief. In some infirmaries the doctors were mainly occupied with surgery and the care of the acutely ill; in others most of the patients were suffering from chronic illnesses. Boards of guardians varied from a progressive attitude to almost complete inertia; these variations could not be justified. In the view of the surveyors, larger areas of organisation were called for. They thought that the administrative County of London was too large a primary unit, just as the borough councils and unions were too small. Meredith Richards and Manby therefore suggested that the infirmaries should be managed in groups based upon borough boundaries, three groups north of the Thames, and two to the south. The special committee on changes in London local government, established by the London County Council, suggested that there should be five non-executive area committees for the purposes of hospital administration, and the council be an to develop the administrative machinery necessary to take conrol.48 Discussions with the guardians made a smooth hand-over possible, and few patients would have noticed the change. The London County Council proved a much less autocratic body than the doctors had feared; consultation with the hospital medical officers was frequent and promotion prospects were better.46 London County Council management The council asked its medical officer and architect to carry out a survey and report on hospital premises. The report on the infirmaries showed that the condition of most left much to be desired. Menzies commented ruefully that all the floors seemed to be breaking up and all needed rewiring. The best were, undoubtedly, Lewisham, Hammersmith, St James’ and St Charles’. The worst were probably St Leonard’s, St Pancras and St Stephen’s.36 The older infirmaries showed little evidence of ordered planning, but those built from 1880 onwards were usually of the H, E, U or V plan, with the administrative block occupying a central position and the wards lying on either side along a main corridor. The London County Council distinguished between hospitals which in essence provided medical treatment and nursing, and institutions for long-term residential care. Menzies told his committee: ‘Many of the deficiencies are attributable to the fact that just as each voluntary hospital is a law unto itself, so hitherto each board of guardians has suffered from a comprehensive legal obligation to provide treatment for all destitute sick persons. Now that the existing poor law boundaries are to be swept away and the area to be considered is the administrative County, a great opportunity is afforded of considering the best way of meeting the needs by rearrangement and regrouping of poor law infirmaries and institutions, so as to utilise them to the maximum degree of efficiency within their limitations.’ Menzies worked on much the same principles as Markham, sixty years before. He suggested the hospitals which might be appropriated by the council under the Public Health Acts, excluding those offering only custodial care. The council approved the list, as did the Ministry, and appropriation took effect on 1 April 1930. Menzies groundwork ensured that on the day a vast new hospital service swung smoothly into action. Hospitals were divided into six categories:
This classification meant that some residents who were not really ‘sick’ occupied beds in acute hospitals, and it took time to transfer them to appropriate institutions. Indeed, it was not clear to the council whether it was best to separate the acute and chronic sick. The council decided that a hospital standard of care should offered to all, including the chronic sick, the aged and the infirm. The council’s management of its hospital service
The nature of the hospitals
which had passed to the council varied widely, as did the
quality of the staff LCC and voluntary hospitals in London, 1931
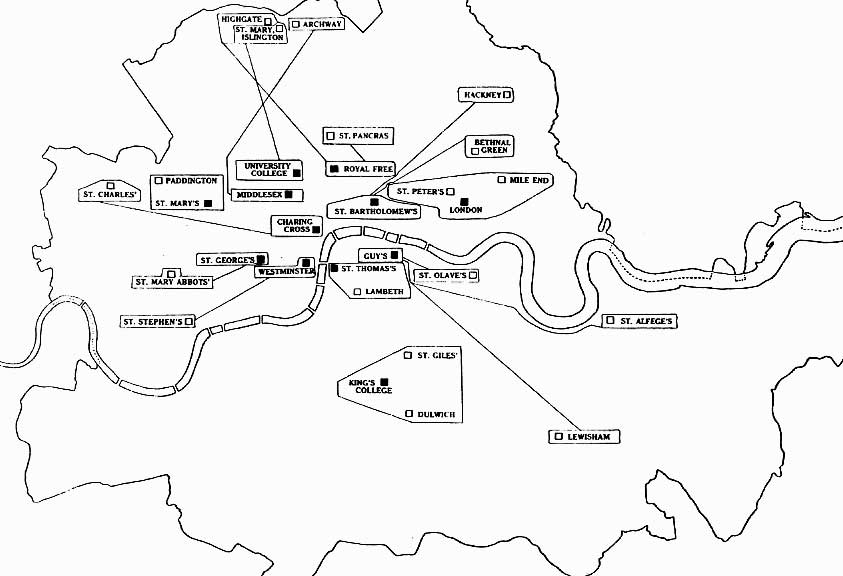
The council’s approach to the provision of outpatient care also differed from that of the voluntary hospitals. The London County Council relied in the first instance on its district medical officers, believing that there was no point in providing an outpatient department to do work that could be done equally well by its district medical and nursing services. The purpose of the hospital was to fill gaps in the district service, providing medical officers and the follow-up of cases discharged from hospital. None of the council’s hospitals allowed patients direct access to the hospital services, as did the voluntary hospitals. The voluntaries justified the policy of ‘an open door to the sick poor’ by arguments which had little appeal for the council. These included distrust of the general practitioner as a sifting mechanism, the provision of clinical material for students, a facility for poor people who had no doctor or who did not wish to see the council’s district medical officer; and the usefulness of the outpatient department as evidence of the popularity of the voluntaries when appeals for support were made. The council’s management style was centralist, based upon a belief in discipline, system and standardisation. The motive was laudable - a desire to see a rapid improvement in the state of the hospitals, and to enforce economy in the provision of services. However the council’s passion for meticulous supervision soon brought it into conflict with the London boroughs and professional organisations. Local hospital committees had few powers and were run by junior staff from County Hall. Decisions involving money, however little, went to the Central Public Health Committee and its successor the Hospital and Medical Services Committee. Each hospital was seen as only a small part of a very large service and neither the local staff nor the hospital committee had a budget or could take decision on matters of policy. Meat was bought centrally at Smithfield, scalpels and syringes were purchased on a central contract, and the minutes of the County Hall committees reveal a mixture of major issues and a welter of trivia. Two or three times a week the committee would deal with matters of moment like the cost of meals of an individual relief nurse, the length of sick leave granted to a junior doctor, or the admission to the obstetric practice of St Mary Abbots, Kensington, of a couple of medical students. Doctors and nurses were responsible to County Hall through the local medical superintendent. The London County Council said that a proper balance had to be maintained between ‘centralised control and devolution of responsibility to “local” centres’. The council thought it had the balance right but few others agreed. Fully aware of the progress being made in all branches of medical science, the council wished this to be reflected in its hospitals. It believed that a hospital which ‘stood still’ was in fact regressing and that money could be saved and efficiency would rise as a result of investment. From 1933 onwards the council’s annual reports recorded the progress which had been made. Between 1934 and 1939 £4 million was spent on hospital improvements. Hospital construction was examined to determine the best policies to follow in renovating buildings. A study of the relative costs of various types of hospital construction was in favour of semi-permanent buildings which would last up to sixty years, being cheaper and more adaptable to changes in medical practice. The Hospital Standards Committee considered the various types of equipment - artery forceps, waterproof sheeting, sanitary fittings, baths and washbasins - and recommended the type to be used. The way in which the departments of a typical 500 bed hospital might be arranged to facilitate effective working was also studied.51 Even hospital names were standardised. In some cases the names were out of date and the possibility was considered of using the names of saints, kings or persons with local associations instead. The officer concerned felt it ‘desirable to adopt some uniform system of nomenclature’, and as some of the transferred hospitals were already named after saints, he found saints’ names for the others. Because saints were not to be duplicated within the administrative county, he sought associations with local parishes. So Plumstead and District Hospital became St Nicholas’, and St Charles’ and St Alfege’s, among others, were given their names. Nursing was a particular problem. The staff transferred from the guardians exceeded 9,000, employed in no fewer than 78 grades. A matron-in-chief was appointed, responsible to Dr Menzies (now Sir Frederick Menzies). He was of the opinion that the only way to create a permanent and efficient nursing staff with a sense of dignity and pride in its work was to make it responsible to a woman of the same status as the principal medical officers — a development which the officers did not view with unqualified approval. Some hospital matrons began to regard themselves as independent of the medical superintendent, and the senior doctor and nurse in a hospital might not be on speaking terms. The London County Council’s service had its strengths and weaknesses. In the face of its impressive achievement any criticism seemed carping, not least because the qualities of Sir Frederick Menzies were a guarantee that matters would not go badly wrong. In 1934-5 Dr Carnwath, of the Ministry, carried out an exhaustive survey of the public health services provided by the council, describing the problems which the council had faced and the way they were being tackied.36 An abbreviated version of his report appeared in the report of the Ministry of Health for 1934-5. The Minister congratulated the council on its enlightened policy and upon the highly efficient organisation built up by Sir Frederick Menzies for overall planning and control of the hospital and medical services. The council was so pleased that it had the appropriate section of the Ministry’s report reprinted as a separate publication. Voluntary hospital and county council cooperation Under section 13 of the Local Government Act local authorities were instructed to consult a committee representative of the governing bodies and medical staff of voluntary hospitals ‘as to the accommodation to be provided and the purpose for which it was to be used’. This clause, designed to foster cooperation, was an expression of Chamberlain’s views, had the support of the voluntary hospitals, and was moved in the Upper House by Lord Dawson of Penn. The British Hospitals Association meeting at the Westminster Hospital in November 1928, viewed cooperation mainly as a means of allocating beds in the infirmaries to the staff of the voluntary hospitals, to make the transfer of chronic cases easier. Representatives of the teaching hospitals who met the following month at St Thomas’s welcomed the centralisation of the public hospitals under the London County Council. They thought that their senior staff would be too busy to work regularly in municipal hospitals, but that it would be desirable for more junior staff to do so for a stipend, to avoid a permanent division between two systems of consultant staff. The voluntaries could also provide the council with resident house officers, and would wish to take advantage of the teaching facilities that the municipal hospitals could offer.52 Members of the London County Council did not take kindly to the attitude of superiority sometimes adopted by the voluntary hospitals. Both sides became touchy and began to stand on their dignity. The King’s Fund tried to act as peacemaker, and suggested that the representatives of the voluntary hospitals, when speaking in public, should censor their remarks to avoid unnecessary offence. Ten years later, in his reminiscences, Menzies regretted that the interests of the voluntaries were not represented by the King’s Fund, but by the specially formed London Voluntary Hospitals Committee. The King’s Fund was well established, highly respected and backed by large resources. Had the King’s Fund’s council and the London County Council been able to work directly together, Menzies thought that relationships would have been much better. As it was joint discussions were a failure from the start. The London Voluntary Hospitals Committee was chaired by Lord Riddell, president of the Royal Free Hospital, who suggested at the first joint meeting with the London County Council that the best policy for the LCC would be to devote itself to the care of the chronic sick, the aged and the infirm, and to make appropriate financial grants to the voluntary hospitals so that they might deal with the acutely sick. Sir Frederick Menzies did not believe that this was the unanimous view of the London Voluntary Hospitals Committee, but its chairman was not a man inclined to encourage colleagues to speak. Similarly the voluntary hospitals did not wish the London County Council to make significant improvements to its hospitals without prior consultation with the voluntaries.54 To make such propositions to the greatest municipal hospital authority in the world was a little tactless, and the attempt to dictate its hospital policy was greatly resented by some council members. It was made clear that while the council might feel disposed to notify the Voluntary Hospitals Committee of proposals involving a substantial increase in accommodation, it would make its own decisions. Lord Riddell thought this was unsatisfactory, and that the council intended to go its own way and develop its service irrespective of the voluntaries. Nevertheless a two-way exchange of information was maintained. The council informed the voluntary hospitals of its proposals. The voluntary hospitals commented upon them, supplying in return details of their own plans.55 The London County Council was proud of its achievements in education and housing and intended to make a similar success of its hospital service. Believing that cooperation with the Voluntary Hospitals Committee would be difficult, it worked with individual hospitals, especially those with medical schools. The medical schools were particularly short of obstetric experience, and the facilities of council units were made available. Sir Frederick Menzies also devised a scheme which linked county council infirmaries to the teaching hospitals. After discussions with the London Voluntary Hospitals Committee the London County Council agreed that ‘facilities should be afforded at its special and general hospitals for demonstrations to medical undergraduate and postgraduate students, on the understanding that the council bore no expense and that the work of the hospitals was not impeded’. In January 1933 Sir Frederick Menzies reviewed the arrangements which already existed with KCH, UCH, St Mary’s and the Royal Free, and held discussions with the twelve London deans about the facilities they might require. The scheme he developed was approved by the council, permitting 12-15 students to attend for demonstrations several times a week.56 Sir Frederick’s scheme was based upon geographical relationships, and was illustrated in the report of the Voluntary Hospitals Committee by a sketch map. It is not surprising that the associations which were established in the 1930s persist to this day. The London County Council was worried initially that an arrangement with a teaching hospital might mean that it would have to look to the hospital for consultant staff. The deans thought that this would be desirable but not essential. Nevertheless they were worried about the quality of teaching students would receive, and students were therefore often taught by a visiting consultant rather than by one of the council’s own medical staff. Rules were laid down and the teacher had to select his cases from a list provided by the medical superintendent, and no impression was to be given at the bedside ‘which might convey a wrong impression to the patient as to his diagnosis or treatment’. The arrangements proved satisfactory and all schools save The London (where adequate facilities already existed) took advantage of the scheme. The senate of the University of London ‘expressed their deep appreciation of the action of the Council in making such important additional facilities available’.57
The London County Council and the Voluntary Hospitals Committee agreed that the council should make no general grants of capital or revenue to individual hospitals without first approaching the committee, but the council might make specific arrangements with individual hospitals for services rendered. A joint survey of hospital provision in London was undertaken. Published in two parts, one for the voluntaries and one for the municipals, the survey’s maps and geographical analysis of patient flows brought the hospital provision for London into focus and enabled the voluntaries to point out that 37% of their patients came from outside the administrative county. National relationships of the hospital systems Local authorities resented the fact that whilst they were obliged to consult the voluntaries under the 1929 Act, there was no reciprocal obligation. In London a mechanism had been created which brought the two sides together, at least in a formal sense. Sir George Newman, chief medical officer of the Ministry of Health, took cooperation as his theme when he addressed the conference of the voluntary hospitals in 1934. Sir George favoured a cooperative hospital system of ‘unity rather than uniformity ... a practical compromise between collectivism and individualism’, rather than placing all hospitals, both voluntary and municipal, on the basis of rates and taxes. Lord Riddell agreed that there must be no jealousy between the two services and admitted that the voluntaries had taken a long time to appreciate the enormous changes brought about by the Local Government Act. Sir Ernest Morris of The London Hospital said that the voluntary hospitals were worried as they had known for a long time that the unsystematic voluntary hospital system could not possibly provide all that was now required of a health service. It would be unable to meet the recommendations either of the Labour Party or Lord Dawson’s consultative council, which said that services ought to be available to everyone. That fear must be mastered - there had been problems enough in the past and they had been overcome.59, 60 Joint survey of medical and surgical services in the administrative county of London, 31 December 1931
The survey excluded services for the mentally ill and handicapped. Source Joint survey of medical and surgical services in the administrative county of London, prepared by the Voluntary Hospitals Committee and the London County Council, two volumes. London, P S King and Son, 1933. The local authorities, however, now had a unified and effective hospital administration, and could confer the power to negotiate upon their representatives. But with whom could they talk? The voluntary hospitals seldom authorised anybody to speak on their behalf, and the Hospitals Year Book of 1932 urged them to strengthen their machinery for consultation so that they could provide a considered and collective view. The days of ‘more or less undisturbed tranquility’ were over and a hospital which made an error in its planning delivered a blow to the voluntary system as a whole.61Hospitals should now act as members of a system with a common policy. In its financial review of 1935 the Hospitals Year Book pointed out that the income of the voluntary hospitals was relatively inelastic, while the enthusiasm of ‘spenders of other peoples’ money’ was setting a standard in the municipal hospitals which it would be hard to match. The London Voluntary Hospitals Committee It was generally known that the London County Council would have preferred to have dealt with the King’s Fund directly, instead of with the Voluntary Hospitals Committee. The LCC treated the committee rather as it treated deputations, in a manner which lacked the open trust of those working together for a common purpose. Relations improved in 1935 when the committee was reconstituted under a new chairman with new officers, but it was too late. It never became a potent influence or rallying point, devoid as it was of financial resources to persuade or coerce the London hospitals into a common policy. The reconstituted committee was elected by individual hospitals and brought together the London Regional Committee of the British Hospitals Association and the statutory committee with which the London County Council had been dealing, so avoiding the problems of communication between various bodies claiming to represent the London voluntary hospitals. The understandings between the LCC and the committee were codified, and the Ministry of Health accepted the Voluntary Hospitals Committee as the body with which matters of importance to London voluntary hospitals were discussed. In giving evidence to the Sankey Commission, the committee expressed the hope that in the course of time it would formulate the principles of hospital policy in London, and, backed by the King’s Fund, would get the principles translated into action. The secretary of the British Hospitals Association believed that this was sensible, but saw that the only power available was the power of the purse, which the King’s Fund alone possessed. The approved procedure was for the voluntary hospitals to provide early information to the Voluntary Hospitals Committee about substantial schemes, before the press was told. They then had to submit fuller details of proposals which involved substantial capital expenditure, or which produced ‘an important change in the amount, nature, cost or site of the work done’. The committee s object was to ensure that all schemes on which subscribers’ money might be spent were clearly justified by the demand for care, but to avoid detailed enquiries into the need for particular forms of therapy or the precise nature of the accommodation to be provided. It did not wish to trench upon the ‘freedom and initiative that distinguished the voluntary from the municipal hospitals’. The King’s Fund instructed the voluntaries to give it prior knowledge of proposed developments, and to seek the views of Lord Riddell and the Voluntary Hospitals Committee before seeking a grant. Mr Ives, who became secretary to both the Fund and the committee, was circumspect in his dealings with the county council. He said that he ‘was not sure how far it was desirable to submit to the London County Council statements setting out in detail the inadequacies of individual voluntary hospitals’. When the Royal Free Hospital sought permission to expand by a hundred beds because of its long waiting lists and the many acutely ill patients that had to be turned away, these details were not passed on to the council.63 Postgraduate education and the British Postgraduate Medical School The establishment in London between the wars of a postgraduate medical education centre was a unique innovation. Two ideas were brought together, the need for a national and imperial centre for postgraduate education, as Sir George Newman had advocated23 and the desirability of providing a firm scientific basis for medical development. In December 1919 Sir Bertrand Dawson, at the request of his Consultative Council, impressed upon Dr Addison, Minister of Health, the need for improved facilities for postgraduate education. In October 1920 the chairman of the University Grants Committee (UGC) asked the Minister to form a small committee on postgraduate education in London. There was pressure on the UGC to fund postgraduate education and a number of schemes were under discussion.64 The Minister agreed and appointed a committee chaired by the Earl of Athlone, the chairman of the Middlesex Hospital. The committee was asked to ‘investigate the needs of medical practitioners and other graduates for further education in medicine in London and to submit proposals for a practicable scheme for meeting them’. The Athlone Committee worked fast and considered a wide range of evidence. It held 26 meetings and reported in May 1921 that a school attached to a hospital of at least 300 beds, centrally situated in London, should be devoted solely to postgraduate education. The ‘great special hospitals’ should be closely associated with the school, but it was held that undergraduate and postgraduate education could not easily coexist in the same institution. Little more was done at the time because of the financial problems of the early twenties, but in 1925 the Minister of Health, Mr Neville Chamberlain, appointed a committee of medical men to devise a practicable scheme. Chamberlain chaired the committee himself, and it included his chief medical officer, Sir George Newman, the Presidents of the Royal Colleges of Physicians and Surgeons, Lord Dawson, and Herbert Eason of Guy’s.66 This committee established a sub-group to visit a number of London hospitals. It rapidly eliminated the Westminster and Charing Cross, because of the limitations of their buildings, and the Royal Northern as it was too far from the centre of town. St George’s would have nothing to do with the idea. The Middlesex and St Mary’s appeared more suitable, but the committee decided that all the other teaching hospitals should be asked whether they wished to be considered. Sir George Newman thought it safe to say that there were more undergraduate schools in London than would be required to meet future needs; that the tendency would be to concentrate education into a smaller number of schools; and that there would be no difficulty in sparing one for postgraduate education. On 17 June 1926 letters went to all the teaching hospitals. Within a few weeks, and sometimes within a few days, the proposal had been turned down by University College Hospital, King’s College Hospital, The London, Guy’s and St Bartholomew’s. St Thomas’s and the Middlesex took a little longer to refuse. In almost all cases the idea was rejected because the future postgraduate hospital would be required to give up undergraduate education. St Mary’s was the only hospital willing to consider the proposition, but asked for further details. In the meanwhile, however, the West London Hospital volunteered and an inspection showed it to be a possibility. After consideration, the Minister’s committee concluded that the West London was the only hospital appropriate for conversion and expansion into a postgraduate centre. Further discussions with its board, however, showed that it had little idea of the scope of the scheme and considerable misgivings about its ability to raise the money to support the beds which would be required. The hospital looked to the Ministry to solve these problems. ‘This is not a Board’ commented Sir George Newman, ‘with whom we can go out tiger hunting’. Sir Berkeley Moynihan, the President of the Royal College of Surgeons, shared his concern and suggested that the passing of the Local Government Bill should be awaited. Then, the best poor law hospital in London should be selected and the college built nearby. This would demonstrate that a first class medical school could be attached to a municipal hospital and that the association of a medical school with a state hospital was constructive and advantageous, rather than restrictive and bureaucratic. There would be no need to beg for voluntary subscriptions. Nevertheless talks continued with the West London, the enthusiasm of its board increasing from cool to lukewarm. Although work on the Local Government Bill was taking up a great deal of time, Neville Chamberlain reassembled his committee in November 1928 to consider the next steps. The imminent municipalisation of the infirmaries led the doctors on the committee to repeat the proposal that an infirmary should be used instead of the West London. Sir Berkeley Moynihan saw Neville Chamberlain in private the day before a meeting of the postgraduate committee on 20 February 1929. During the meeting the President of the Royal College of Physicians, Sir Humphrey Rolleston, said that the objection to the West London scheme was that the committee would not be aiming at the best within its reach. The West London was not central, the problem of its existing staff (and its quality) had not been solved, and the scheme might cost as much as an entirely new institution. Sir Berkeley Moynihan said that the West London was not large enough to accommodate all the special departments required, that the medical staff was not of such standing as to be easily assimilated into the new centre, and that alternatives should be explored. Mr Chamberlain read out a letter from Lord Dawson which asked for exploratory talks with the London County Council. The committee discussed the possible use of the infirmaries at Camberwell, Lambeth, Lewisham and Wandsworth and none of the members opposed the idea. Mr Chamberlain agreed at the committee’s request to approach suitable members of the London County Council. In the meanwhile, he would see the chairman of the West London Hospital to inform him of the reservations of the committee about proceeding further.67 The London County Council proved to be willing. A report proposing the association of the new school with the Hammersmith Hospital went to the Cabinet and was presented to Parliament in April 1930. The postgraduate school was to be established at the Hammersmith with the assistance of a government grant.68, 69 Although the idea of using a municipal hospital had been generally supported by the eminent doctors who were members of the postgraduate education committee, it was not to the liking of the London Voluntary Hospitals Committee. While unable to suggest any alternative, it pointed out that the voluntary hospitals were the traditional basis for medical education and argued that expansion into postgraduate teaching would be better conducted in a voluntary than in a municipal hospital. It maintained that doctors with large private practices had the widest clinical experience and best knew the needs of general practitioners. The stimulus of postgraduate education, and the Treasury grant which went with it, should be kept within the voluntary system. If a London County Council hospital became the new centre, its whole-time staff would become university teachers, suggesting that the centre of gravity of even undergraduate teaching might gradually shift to the municipal hospitals, an occurrence which would greatly undermine the voluntary system as the teaching of medicine was one of its main sources of strength and vitality. A further objection was that to place the centre of postgraduate education on the outskirts of London was a fundamental mistake.70 During subsequent discussions with the LCC it was agreed that while the Hammersmith should be well equipped as a hospital, unrealistic standards of provision were not necessary. The quality of the teaching would depend on the quality of the teachers. The economic problems of 1932 led to a reduction in the government grant from £250,000 to £100,000. The scheme came to a halt and the appointment of the dean was delayed. For a time it was feared that the whole project would have to be cancelled, but in November 1932 the chancellor agreed that it could go ahead and the London County Council was informed.71 The council facilitated the conversion of the Hammersmith Hospital into a centre for postgraduate education, matching the government’s grant by one of its own. The British Postgraduate Medical School, as it was called, agreed to meet a proportion of the extra cost which arose from its establishment in relation to the hospital, the LCC and the school sharing the cost of equipment for joint use. The school was opened in 1935, Professor Francis Fraser moving from St Bartholomew’s Hospital to become its first professor of medicine. Some of the intentions of the founders were expressed by King George V at the opening. The school was to be ‘rooted in the ward and the laboratory’ and was to ‘renew knowledge and disseminate it for the benefit of mankind’. Stress was laid upon the contribution to be made to the Commonwealth, and the overseas relationship was underlined by the composition of the governing body. Professor Fraser was later to play a key role in the hospital service of London during the years of war, and in the emergence of the pattern of the National Health Service in the capital. He was able to establish new traditions at the Hammersmith and to ensure that from the beginning the hospital and school were staffed at consultant level mainly by whole-time academics. The voluntary hospital system’s prospects The voluntary hospital system was now on the defensive. During the financial crisis of 1921 its efficiency had been called into question. With the advent of the municipal hospitals in 1929 its very existence was at stake. Between 1928 and 1932 the London voluntary hospitals had increased their beds from 15,900 to 17,100, and treated 16 per cent more inpatients. However the cost per bed was rising and voluntary donations were falling, although the shortfall was made good by increasing payments by patients. In 1932, 85 hospitals succeeded in balancing their books; 60 did not.72 In 1930 Mr Inman, then house governor at Charing Cross Hospital, wrote two articles for the News Chronicle and the Star.73 He said that what was vitally necessary was not a patched up policy but a permanent panacea. Hospitals could not rely on sweepstakes and competitions for their survival. He saw three possibilities: that the depression would end and the financial state of the hospitals would improve; that the state might offer assistance without there being state control; or that the hospitals would be nationalised. He forecast that in ten years every hospital would be state supported and state controlled. That such a statement should be made in the press by the house governor of a teaching hospital alarmed the King’s Fund. The Fund’s council members were sent a copy of the offending articles and their chairman asked the chairman of Charing Cross, Mr Verity, to come to see him. Verity was completely loyal to his house governor, and said that he shared Inman’s detestation of the undignified methods of fund-raising which were in vogue. Inman himself wrote to the Fund expressing his strong support for the voluntary system.74 The seriousness of the hospitals’ financial position led the British Hospitals Association to pass a resolution in 1935 to establish a commission, chaired by Lord Sankey, to examine the administration, management and finance of the voluntary hospitals. The main organisations with an interest in hospitals gave evidence, while the commission considered how the hospitals’ interests could be promoted, their policy developed and their future safeguarded.75 Although the King’s Fund was sympathetic it declined to give evidence, while prepared to answer any ‘definite questions’ which were addressed to it. The commission s report, published in 1937, stated that future prospects were not favourable, and made thirty seven recommendations involving major changes which were considered essential if the voluntary system was to continue. A key proposal was the formation of regional councils to express ‘considered views’ on hospital systematisation. Loyal acceptance of their decisions was expected, even if they were painful.76 Similar proposals had been made sixteen years earlier by the Cave committee.12 The more accommodating spirit now in evidence was inspired both by fear and hope; fear of being driven out of business by the municipal hospitals, and hope of receiving assistance from local authorities or the state. No member of the Sankey commission worked in a special hospital and its report reflected evidence given by the Royal College of Surgeons that special hospitals should be brought into close cooperation with general hospitals, or run as one of their departments.62 This exercise in force majeur did not appeal to the special hospitals, one of whose secretaries protested to the British Hospitals Association. Political and Economic Planning (PEP), a group of individuals interested in the planning of the country’s services, also regarded the case against the special hospitals as ‘not proven.' 77 Although it seldom displayed its power in public, the influence of the King’s Fund was considerable. In 1924 it investigated the problems of the uncoordinated ambulance services in London and the difficulties of obtaining an emergency admission, both of which were complicated by the large number of independent hospital boards and poor law infirmaries governed by guardians whose rules and regulations varied. A hospital economy committee was formed in 1924, during the period of financial crisis, to examine comparative costs, draw the attention of hospitals to excessive expenditure, and consider the explanations offered by the hospitals. This committee also examined the reason why hospital beds might be underoccupied, and the way better use might be made of existing facilities.78 The management of voluntary hospital outpatient departments was the concern of a special committee chaired by Lord Onslow in 1931. The voluntary hospitals’ open door policy continued to attract criticism. The Charity Organisation Society and the British Medical Association gave evidence, as did many of the hospitals. The BMA’s view that outpatient departments should be purely consultative, seeing only those patients referred by general practitioners, was considered impracticable. The introduction of appointment systems was also thought to present too many practical problems, although ways of reducing the time spent waiting for the doctor were suggested.78 In 1936 the Fund explored a suggestion of Mr Gardham, a surgeon at University College Hospital, that a centralised admissions service should be established for the voluntary hospitals. Faced with competition from the London County Council hospitals, the voluntaries needed such a service to ensure that they continued to receive a flow of emergency work, so necessary for medical education. The service would also supply a public need and remove a possible cause for criticism. And so the Emergency Bed Service was born.78 The King’s Fund also continued its work of considering building plans, sanctioning improvements and advising hospitals on new developments. Hospitals could not always be persuaded to make the most sensible decisions, but the wilder ideas were usually extinguished. A hospital which went its own way had little chance of a successful appeal to the Fund if things went wrong.79 Despite financial problems, two major teaching hospitals were largely rebuilt the Middlesex under the chairmanship of Prince Arthur of Connaught, and the Westminster under Sir Bernard Docker. In 1923 a large fail of plaster revealed unexpected defects at the Middlesex. The surveyor’s report showed that the east and west wings were in a dangerous condition. Their foundations were virtually non-existent and wards would have to be closed. The King’s Fund was worried at the prospect of a major appeal at a time of economic crisis and a second survey was carried out at its request to see if remedial works would be possible. The findings were confirmed; the Middlesex really was falling down. The hospital favoured total reconstruction and an appeal was launched to which the King’s Fund made substantial grants. One wing at a time was demolished and rebuilt, and the new building was opened in 1935 by the Duke of York.80 Significant additions were made to many other hospitals. St Bartholomew’s rebuilt its surgical block with the help of the King’s Fund, and launched a much larger appeal for a million pounds in 1929, but without telling the King’s Fund in advance. The hospital expressed its regrets and the Fund accepted the new proposal with good grace. However because of the economic situation the response was poor and the appeal had to be abandoned.81 University College Hospital built a new obstetric hospital which was opened with the customary panache. The secretary wrote to his chairman: ‘I think we might have a big marquee with a platform and accommodation for one or two thousand people. We should also have a band and when the Prince has opened the new buildings the company might re-adjourn to the College grounds for tea and refreshments.’82 Special hospitals were also developing their facilities. Queen Charlotte’s was rebuilt to the west, in Goldhawk Road, a major block was added to the National Hospital for Nervous Diseases, and there was rebuilding at the Gordon, St Mark’s and at the Royal Westminster Ophthalmic Hospital. The medical staff at Great Ormond Street were asked to report on the condition of their hospital, and their highly critical comments led to the construction of the Southwood wing. New architectural principles were applied to the design of the new buildings. Aerial spread of infection was largely discredited and the pavilion plan was abandoned. Instead, compact multi-storey blocks were erected, in part because of the cost of city-centre land. Ward units were smaller and more space was devoted to service departments. An attempt was made to deal with ward infection by partitions and screens, balconies were increasingly introduced, and attention was paid to the problem of noise. It was appreciated that building vertically rather than horizontally would make it more difficult to adapt hospitals to changing requirements, as has proved to be the case.83 Facilities were improved to keep pace with medical science. The King’s Fund established a radium fund and supervised the distribution. Professorial clinical units were introduced. But these developments did not alter the historic concentration of hospitals in central London which was hardly, in the opinion of Political and Economic Planning, the best arrangement under modern conditions.77 The Westminster, St George’s and Charing Cross Hospitals Many hospitals were replanning their services and the King’s Fund was at the centre of all proposals for redevelopment. In 1913 the Westminster had purchased a site on the north side of Clapham Common, the Fund agreeing to make an annual grant towards the payment of interest on the mortgage. Once the war ended the scheme was revived and in July 1919 plans were drawn up for a new hospital. However, the Westminster’s medical staff now preferred an alternative — amalgamation with King’s College Hospital at Denmark Hill. They feared that the money available would not be enough to build and maintain a new Westminster Hospital large enough to contain a full range of clinical facilities and achieve recognition as a clinical medical school. The King’s Fund discussed the facilities which might be made available to the Westminster Hospital at Denmark Hill with Lord Hambledon, chairman of King’s College Hospital. Although only 360 of the 600 beds originally planned had been built, Lord Hambledon said that half of them could go to the Westminster. Some expansion would be comparatively easy and the name ‘The King’s Westminster Hospital’ would be quite acceptable. Having considered the options open to the Westminster, the King’s Fund continued to prefer Clapham and suggested that the Westminster might consider amalgamation with another hospital on that site. But as the cost of the Clapham scheme was high the Fund agreed that if it became too expensive and the need to move was pressing, Denmark Hill might be reconsidered.84 Neither proposal proved practicable and the Westminster’s Broad Sanctuary building had to be upgraded, to the distress of Lord Knutsford who thought it a ‘ghastly waste of money’ and the loss of a great opportunity to achieve either the removal of the Westminster or its amalgamation with another hospital. There matters rested until 1933 when the Westminster was offered the Horseferry Road site. A scheme for amalgamation with St George’s was then considered, but St George’s felt that the Westminster was paying too much for the land and did not like its position. The Westminster had to go it alone. The King’s Fund was kept fully informed throughout the complex negotiations and the land was not purchased until its approval had been obtained. The Westminster Hospital’s appeal brochure was edited by the Fund before it was issued.85 Charing Cross was another potential partner for the Westminster. It had long been accepted that the Charing Cross site was inadequate, without room for expansion. The Fund used its influence in 1936 to prevent Charing Cross rebuilding at the Adelphi because of the high cost of the site, and pointed to the existence of enough ground in Horseferry Road to build a 400 bed hospital next to the Westminster, but Charing Cross would not agree to abandon its separate existence. The Westminster’s new buildings were opened in April 1939, and were hailed as a new departure in hospital planning. Outpatient and inpatient departments were related to each other on each floor, to make progressive patient care easier. The King’s Fund later agreed to an alternative scheme for Charing Cross Hospital which was proposed in 1938. It would have provided 320 ordinary and 80 private beds at the north end ofShaftesbury Avenue, to which neither University College Hospital nor the Middlesex made any objection.86 St George’s was also slow in coming to any firm conclusion. For thirty years it had vacillated over rebuilding at Hyde Park Corner or attempting to sell the site - difficult because of divided ownership - to finance removal. In January 1935 it was agreed that the hospital should be rebuilt where it was. The council of the King’s Fund viewed the proposal with disquiet, but acquiesced after the views of all its members had been canvassed. The Fund’s approval was given in February 1935 and an appeal was launched. HRH the Duke of Kent contributed the money collected for his wedding gift, and signed the appeal brochure which was issued the following year.87 Dr Hugh Gainsborough, speaking at the hospital’s annual dinner in 1937, deplored hurry. Hospitals had to be carefully planned; ‘plan slowly and build quickly’ was his message. The architect published his plans for a twelve storey building in March 1939, but the planning had been too slow. The new hospital could not be constructed because of the outbreak of war.88 The architect, however, was subsequently involved in the postwar redevelopment of Guy’s. The King’s College Hospital crisis In 1930 King’s College Hospital, in dire straits, had approached the London County Council for assistance. The London Voluntary Hospitals Committee asked King’s not to make its request for financial help public. The county council refused a general grant-in-aid. Again in 1938 the hospital’s financial position began to deteriorate. This time the King’s Fund agreed to make an emergency grant of a pound for every pound the hospital could raise above its average receipts in previous years, with an upper limit of £5,000. In due course this sum was provided. The hospital also asked the county council that year to receive a deputation.89 It was made clear to the council that the hospital did not wish the Voluntary Hospitals Committee to act as an intermediary. The deputation, led by Lord Hambledon, presented a memorandum outlining the origin of the Denmark Hill development. Only two thirds of the beds originally planned had been built, the council was already using one ward as an adjunct to the Maudsley and King’s was prepared to make a further ward available to the council should it wish to expand its acute services in south London. King’s also suggested a joint approach to the provision of acute hospital services by the council and the hospital and pointed to the availability of adjacent land for new building. Questioning made it clear that Lord Hambledon was afraid that if matters did not improve, more wards would have to be shut. The hospital was, therefore, seeking council assistance to open and run wards which it could not itself finance, a course of action which would be contrary to the agreement which obliged the council to pay only for services rendered. The problem was referred to the London Voluntary Hospitals Committee. Conferences and delegations After King’s had been to see the LCC, Sir Frederick Menzies wrote in confidence to the Minister of Health, drawing attention to the serious revenue problems of some of the teaching hospitals. He believed that St Thomas’s and the Middlesex might be on the rocks within 12-18 months. Other hospitals were in need of capital for modernisation schemes, like The London, St George’s, Charing Cross and Guy’s. The forthcoming pay recommendations of the Inter-Departmental Committee on Nursing Services were likely to increase costs and the voluntary hospitals would be hard hit, and quite a lot of them would be seriously damaged.
Menzies felt that it would be disastrous if the
great hospitals had to close beds, or fell
behind in medical science - their
medical schools and their national role as
teaching centres were of inestimable value. He
therefore suggested a royal commission to
explore the problems urgently and report
rapidly. The chief medical officer consulted the
King’s Fund and the principal of the University
of London, Herbert Eason of Guy’s. Both believed
that help was necessary and supported the
proposal for a commission. However, they thought
the problem a national one, and that the
solution would be a hospitals board to provide
grants to all teaching hospitals, just as the
University Grants Committee funded the medical
schools. For the time being they thought that
the most likely source of money for London
hospitals was the LCC, in view of the sympathy
Menzies was showing, and in spite of the
apprehension of the hospitals about undue local
authority control.90, 91In Menzies’
view the problem was mainly a London one. He
said that there was no territorial pride in the
County of London ‘and the Londoner, as a
Londoner, did not care twopence about the future
of the voluntary hospitals’. There was to be no royal commission but in June 1938 the King’s Fund convened a private conference of the twelve teaching hospitals to consider their high costs. Over the years their costs had risen considerably and in 1938 they were 200 per cent higher than in 1913. The proportion defrayed by the King’s Fund had fallen from around 15 per cent to 3 per cent, but the King’s Fund figures for the period 193337 showed that, taken as a whole, the voluntary movement in London was not in too bad shape. The Hospitals Year Book, however, had drawn attention to the marked differences in maintenance costs of the London hospitals and those in the provinces. In 1935 the annual expenditure per bed in the London hospitals was £236.1 whereas in provincial hospitals it was only £137.9. Costs were slowly rising, but the differences remained each year. The Fund’s conference agreed that the high costs of the teaching hospitals were due to:
Supported by the Fund, the representatives of the teaching hospitals submitted a memorandum to the Minister of Health, Mr Walter Elliot, on the case for a state grant to the London undergraduate teaching hospitals. While paying tribute to the help received by the medical schools from the government, the memorandum pointed out that the provision of clinical facilities included much more than teaching and teaching equipment. Heavy expenditure fell upon the hospitals. The Minister received a deputation in November 1938 but was non-committal. In July 1938 representatives of the voluntary hospitals suggested another conference with a wider attendance. It would consider three main proposals to place the hospitals on a sounder financial basis: first, a regional grouping of hospitals, pooling their resources; the second, subsidy by the state or the local authority; third, an extension of the contributory and hospital savings schemes which had brought much relief to the hospitals already. During informal discussions a central advisory board for London was proposed, chaired perhaps by Lord Dawson, with a membership from the Ministry of Health, the London County Council and the King’s Fund. As the financial crisis worsened the voluntary movement pressed for a conference. The London County Council saw no grounds for holding one but was prepared to attend without commitment. It finally took place in January 1939 as a confidential discussion between the Ministry, the King’s Fund and the council, and was held at the Ministry of Health.92 Everyone agreed on the virtue of cooperation and that it had been more successful in other large cities than in London. Lord Dawson thought that it would be folly to displace either of the two systems, voluntary or municipal, but an effective service for the County of London needed planning. He therefore advocated an advisory board to classify hospitals, identify places where the services needed strengthening, and prevent overlap. The LCC and the King’s Fund could look to such a board for advice in making their allocations. Lord Dawson hoped for additional money from the state, but said privately that the voluntary hospitals should pool their resources and help each other. The King’s Fund pointed out that the London voluntary hospitals were 146 separate units and a hospital in distress could not draw upon the assets of a more fortunate institution. The Fund’s ability to adjust inequalities depended on its income, then £300,000 a year; salvation could only come from the state or the LCC. Herbert Eason, speaking for the university, paid tribute to the high quality of care and organisation in the London County Council system. He said he would prefer council money and supervision to that of the state. The voluntary hospital representatives as a whole wondered whether the time had not come to review the question of capital and maintenance contributions from the council. Speaking for the council, Herbert Morrison said that it could spend with advantage far more money on its own hospitals than it was doing. But the rate-payers might rebel and it was his business to win elections, not to lose them. The voluntary hospitals already received some £160,000 a year for contracted services. Although he conceded that some extension of this principle was possible, he did not think that the council would embrace the idea of block grants that the voluntary hospitals were now suggesting. Substantial public finance for the voluntary hospitals would reduce the subscriptions they received. Neither did he personally favour a joint advisory board if the voluntaries were to retain a proper sense of their financial responsibilities. Were all 146 voluntary hospitals justified? If some of those which could not be run effectively and efficiently were eliminated, the King’s Fund could restrict its contributions to the best. The council was sympathetic and wished to be helpful, but difficult problems were involved. Other council members pointed out that the teaching hospitals, which were in the deepest trouble, were national institutions and a problem largely for the state rather than London. Speaking on behalf of the council’s finance committee, a member pointed out that the council bore the burden of all the mental hospitals and the care of the chronic sick, problems with which the voluntary hospitals were not concerned. If teaching hospitals cost more than other voluntary hospitals, was it not for the state to meet the difference? Sir Frederick Menzies returned to the theme of hospital planning; an appeal was to be launched to rebuild St George’s on site and Charing Cross was considering removal. The rebuilding of hospitals and medical schools was a question of major importance, to which careful thought must be given. The King’s Fund pointed out that it was the smaller hospitals which were solvent, and to eliminate them would be difficult. Herbert Morrison, sensing that there was increasing pressure for a financial commitment he was unable to give, said that the problem could be taken no further for the time being.92 The Minister, when questioned in Parliament subsequently, could give no more than a non-committal reply about the outcome of the conference. The attempt to create an advisory board, and to persuade the Council to contribute more money, had failed. A county council spokesman was quoted in the press as saying that the addition of the costs of the voluntary hospitals to its own budget would add is 1s 5d to the rates.93 Both the London County Council and the voluntary hospitals were willing to see the state make grants. But at least one Ministry officer thought that if state grants perpetuated the existing pattern of medical education that would probably be a mistake. He felt that the organisation was far from ideal, for there were many medical schools and some of the hospitals with which they were associated were ridiculously small. Emergency planning But other matters were now on people’s minds. The risk of war with Germany was rapidly increasing and the Ministry, the council and the Voluntary Hospitals Committee had to concentrate on emergency planning. The first task was to determine how many beds the hospitals could hold in time of war. In December 1937 Sir Frederick Menzies and Professor Dudgeon of St Thomas’s, representing the voluntary hospitals, were called to the Ministry and told that there was to be a national survey of ‘anything called a hospital or a Poor Law institution’. Shortly afterwards, with their assistance, questionnaires were sent out to the hospitals, which were subsequently visited by a Ministry inspector. Preliminary results were available a month later and the final draft was circulated in May 1938 Summary of available beds in London hospitals
Menzies and his colleagues agreed that, all things being equal, the extra beds which would be needed should be placed on the periphery of London, on ground adjacent to the main roads out of town. A policy of dispersal was safer because ‘there was the certainty that several of the London hospitals would be put out of action’. Menzies envisaged the division of London into sectors, three north and three south of the Thames.94 In May 1938 attention was turned to the problems of dealing with mass casualties from intensive bombing, casualty evacuation, and the transport of those patients who could be moved from beds in central hospitals. A committee was established under the chairmanship of Sir Charles Wilson (afterwards Lord Moran), which reported two months later. The number of casualties predicted was high - an estimate of 30,000 per day for several weeks. It was therefore agreed that some 50,000 beds would be needed in the inner zone, and that rapid evacuation of casualties would be necessary. It was suggested that the whole of the region should be divided into five segments radiating from the centre, with the general idea that the hospitals in the inner part of each segment would clear their casualties to the outer part.95 A further group was established to examine the way in which a series of temporary hutted hospitals could be created to increase the number of beds available. Driven by Dr John Hebb, a rough diamond transferred from the staff of the Ministry of Pensions, plans were well in hand by July 1939 to provide a ring of hutted hospitals on the periphery of London.96 Equipping them proved difficult in the face of the demands from the armed services. The Ministry turned to Eric Salmon, Clerk to the London County Council, who asked how much might be spent. ‘Whatever it costs’ was Evelyn Sharpe’s answer, and the highly efficient supplies department of the council did the rest. With the establishment of the Emergency Medical Service, Sir Frederick Menzies took early retirement. Other committees considered transportation, the conversion of buses into ambulances, and the way ambulance trains might be stabled and routed. Labels were printed to attach to patients, indicating the hospital to which they were being evacuated. Teaching hospitals examined the way in which clinical information might be passed to receiving hospitals without risking the permanent loss of case notes. On 31 August 1939 the Ministry of Health gave the order to the railway companies to proceed with the assembly and preparation of thirty-four casualty evacuation trains. A fleet of Green Line buses was requisitioned. They were in position on 4 September. Hospitals divided their patients into those fit to go home, those fit to move and those who had to stay where they were. The evacuation of patients then began.97, 98 1 Honigsbaum F. The division in British medicine. London, Kogan Page, 1978; and Newman Sir George. The building of a nation’s health. London, Macmillan, 1939. 2 Report on the transfer of functions of poor law authorities. (Chairman: Sir Donald Maclean). London, Ministry of Reconstruction, 1918; and Reconstruction problems no 23, I & II. The present problems and the Ministry of Health. London, Ministry of Reconstruction, 1919. 3 Moore B and Parker C. The case for a state medical service restated. Lancet, 1918, ii, p 85. 4 Shaw Lauriston E. Medicine and the state. Lancet, 1918, ii, pp 87—90. 5 Conference of the British Hospitals Association. Lancet, 1918, ii, pp 397, 566; and Should voluntary and poor law hospitals combine? The Hospital, 1920, 68, pp 63 1—2. 6 Dawson Sir Bertrand. The future of the medical profession. (Cavendish Lecture). Lancet, 1918, ii, pp 83—5; and Watson F. Dawson of Penn. London, Chatto and Windus, 1950. 7 Burdett H C. Hospitals and asylums of the world, volume 3. London, J and A Churchill, 1893. 8 Burdett H C. Ed. Hospitals and charities, 30th edition. London, The Scientific Press, 1919. 9 The organisation of preventative and curative medical services. London, Labour Party, 1918. 10 The capital of the central funds. The Hospital, 14 August 1920; King’s Fund A/KE/1 10. 11 The future of the voluntary hospitals. Lancet, 1920, i, pp 613, 719, 873. 12 Great Britain, Ministry of Health. Final report of the Voluntary Hospitals Commission. (Chairman: Lord Cave). London, Ministry of Health, 1921. Cmn 1335. 13 PRO/MH/58/165. 14 The Times, 5 December 1921. 15 King’s Fund A/KE/303/2. 16 The Labour movement and the hospital crisis. London, TUC and the Labour Party, 1922; also Lancet, 1924, i, p 928. 17 Special conference on the hospital problem. BMJ Supplement, 1924, pp 213—23 and Labour Party; also Lancet, 1924, i, pp 923—928. 18 The need for further voluntary hospital accommodation in London. London, King Edward’s Hospital Fund for London, 1924. 19 Great Britain, Ministry of Health. Report by the Voluntary Hospitals Conimission on voluntary hospital accommodation in England and Wales. (Chairman:The Earl of Onslow). London, Ministry of Health, 1925. Cmnd 2486. 20 PRO/MH/73/42. 21 PRO/MH/80/24. 22 King’s Fund A/KE/308(5); and Lancet, 1937, ii, pp 1467—8. 23 Newman Sir George. Notes on medical education in England. London, HMSO, 1918. Cmnd 9124; and The medical curriculum. The Hospital. 10 July 1920, p 382. 24 Osler Sir William. The hospital unit in university work. Lancet, 1911, i, pp 211, 249. 25 Parliamentary Debates (Hansard) House of Commons 16 April 1888, column 1360. 26 PRO/MH/78/72. 27 Report to the London County Council on the health functions of local authorities and other bodies in London. No 1979. London County Council, P 5 King and Co, 1919; and The Medical Officer, 1920, pp 12, 14. 28 London County Council Minutes, 18 May 1920; and The LCC and the MAB. Lancet, 1920, ii, pp 359—360. 29 Annual report of the Metropolitan Asylums Board, 1925—6. 30 PRO/MH/53/54. 31 Newman Sir George. Fifty years’ progress in public health. Address to the Royal Sanitary Institute. London, Royal Sanitary Institute, 1925. 32 King’s Fund A/KE/109. 33 PRO/MH/58/160. 34 Chamberlain N. Speech to the autumn dinner of the British Medical Association. British Medical Journal, 1927, ii, supplement p 155. 35 Eason H. Co-operation between voluntary and municipal hospitals. British Medical Journal, 1927, ii, p 575. 36 PRO/MH/66/155. 37 Retirement of a public servant. Lancet, 1939, ii, p 839. 38 King’s Fund A/KE/68. 39 PRO/MH/58/165. 40 PRO/MH/79/5 12. King’s Fund papers on co-ordination A/KE/1 15. 41 Relations between voluntary hospitals and municipal hospitals under the local government bill. London, King’s Fund, 1929; and A/KE/68. 42 Great Britain, Ministry of Health. General circular on the Local Government Act 1929. London, HMSO, 1929. (Circular 1000). 43 Menzies F N K. The Local Government Act 1929. Lancet, 1929, ii, p 737; and Address to the British Hospitals Association, Lancet, 1924, i, p 1331. 44 Silkin L. The new public health organisation of the London County Council. London, London Labour Publications, 1930. 45 Coleman R E and Daley W A. The development of the hospital services with particular reference to the municipal hospital system of London. Proceedings of the Royal Society of Medicine, 1942, 35, pp 741—752. 46 Watkin P J. Lambeth Hospital: fifty years retrospect. London, Buck and Wooton, 1954. 47 Meredith Richards and Manby. Report on the institutional treatment of the sick in London. Ministry of Health, 1928. (unpublished). 48 Minutes of the London County Council, 16 July 1929. 49 The LCC hospitals — a retrospect. London, LCC, 1949; and Menzies Sir F. Memorandum on the LCC municipal hospital service. August 1941. Unpublished. Available DHSS Library. 50 Minutes of London County Council, 18 March 1930; andLancet,1932, i, pp 160—2, 427—8. 51 Annual report of the Council, Part IV. Public health general and special hospitals. London County Council, 1932. 52 UCH Archives /A1/23. 53 King’s Fund A/KE/117; and A/KE/38. 54 PRO/MH/77/25. 55 King’s Fund A/KE/203. 56 Minutes of the London County Council, 28 January 1933. 57 Minutes of the central public health committee of the London County Council, 1934. 58 Joint survey of medical and surgical services in the County of London, Part I, London voluntary hospitals committee. P 5 King and Son; Part II, London County Council, 1933. 59 Conference on the voluntary hospitals. London, British Hospitals Association, 1934. 60 PRO/MH/58/165. 61 PRO/MH/58/164. 62 Working papers of the Sankey Commission. British Hospitals Association, 1936. In the custody of the library of the London School of Economics; also PRO/MI-1/580/320. 63 King’s Fund A/KE/438 (a) and (b). 64 PRO/MH/73/49 and PRO/MH/58/40. 65 Great Britain, Ministry of Health, Postgraduate Medical Committee. Report of the postgraduate medical committee. (Chairman: the Earl of Athlone) London, HMSO, 1921. 66 PRO/MH/58/24. 67 PRO/MH/58/21. 68 PRO/MH/58/14, 58/28, 79/390. 69 Great Britain, Ministry of Health, Postgraduate Medical Education Committee. Report of the Postgraduate Medical Education Committee, session 1929/30. (Chairman: Arthur Greenwood). London, HMSO, 1930. Cmnd 3535. 70 King’s Fund AIKE/117. 71 PRO/MI{/58/6; and Minutes of the London County Council, 14 March 1933. 72 The hospitals in the last five years. London, King’s Fund, 1933. 73 Inman P. The voluntary system. News Chronicle, 29 July 1930; and Star, 21 November 1930. 74 King’s Fund A/KE/246/6. 75 PRO/MH/58/164; and The Times, 9 November 1935. 76 Report of the Voluntary Hospitals Commission. (Sankey Report). London, British Hospitals Association, 1937. 77 Report on the British health services. London, Political and Economic Planning, 1937. 78 Outpatient departments, King’s Fund A/KE/47 & 131; Lancet, 1932, i, p 29; Economy Committee, King’s Fund A/KE/33; Report on unoccupied beds, King’s Fund 1930; and Emergency Bed Service, King’s Fund A/ KE/25 and 437. 79 Conference on the voluntary hospitals. British Hospitals Association, London, 1934. 80 King’s Fund A/KE/523(6). 81 King’s Fund A/KE/531(2). 82 University College Hospital archives on obstetric hospital. 83 Memorandum on the construction of voluntary hospitals. Voluntary Hospitals Commission. London, HMSO, 1926. Modern Hospital Construction. Lancet, 1932, i, pp 196-7; and The Architect’s Journal, Special Hospital Number, 24 June 1937. 84 King’s Fund A/KE/25 1/4. 85 King’s Fund A/KE/536/3. 86 King’s Fund A/KE/514/11. 87 King’s Fund A/KF1531/4. 88 The new St George’s. Lancet, 1937, ii, p 885; and Lancet, 1939, i, pp 599—601. 89 King’s Fund A/KE/117, 118, 539(18). 90 PRO/MH/79/5 13. 91 PRO/MH/80/24. 92 PRO/MH/79/5 13. 93 PRO/MH/80/24. 94 PRO/MH/76/99. 95 PRO/MH/76/128. 96 PRO/MH/76/242. 97 PRO/MH/76/248. 98 Town into country. Lancet, 1939, ii, p 605.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
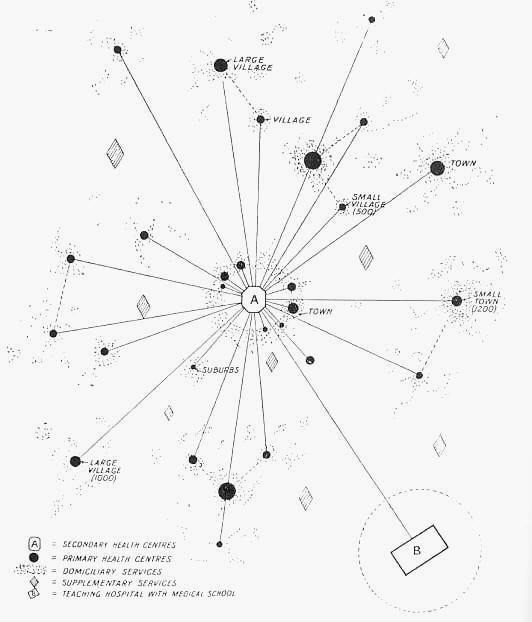
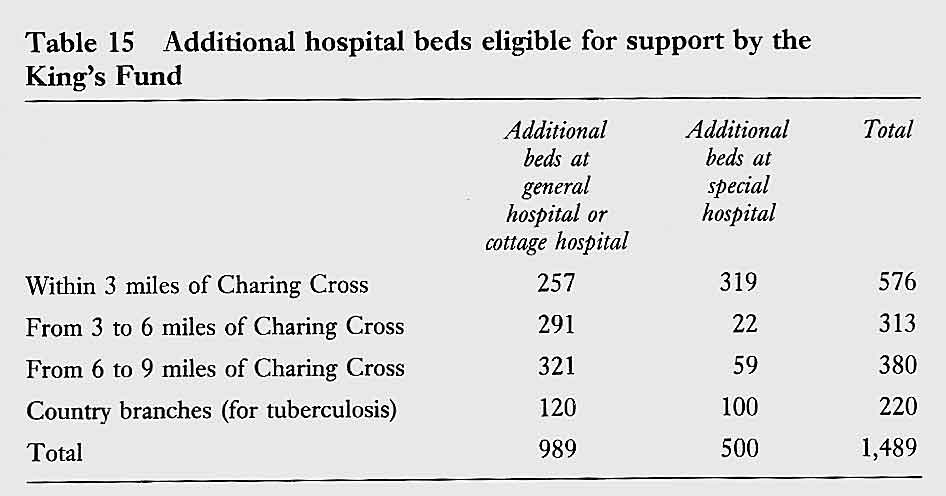
 and
recommended as temporary assistance a state grant of a million
pounds with a further grant the following year. The committee
proposed the formation of a Voluntary Hospitals Commission to
supervise the distribution of the grant, acting on the advice of
local hospital committees.12
and
recommended as temporary assistance a state grant of a million
pounds with a further grant the following year. The committee
proposed the formation of a Voluntary Hospitals Commission to
supervise the distribution of the grant, acting on the advice of
local hospital committees.12 tern
of hospitals, clinics and dispensaries already in existence.21
tern
of hospitals, clinics and dispensaries already in existence.21 and
their terms of service. The assimilation of 75 hospitals
with 40,000 beds and a workforce of 26,000 into a single
organisation was a task of the first magnitude which took
several years to complete. The achievement was impressive by
any standard.49 50
and
their terms of service. The assimilation of 75 hospitals
with 40,000 beds and a workforce of 26,000 into a single
organisation was a task of the first magnitude which took
several years to complete. The achievement was impressive by
any standard.49 50